eGI值——体外模拟测试GI
人体实验是测试血糖生成指数(Glycemic index, GI)的金标准方法,但试验过程复杂,操作难度大且费用较贵。当我们想快速大量地筛选样品时,金标准就不太适用了。那如何快速预估样品的GI值呢?
借助体外消化模型就可以解决这一难题,但体外测试得到的数值并非GI值,而称为估计血糖生成指数(Expected glycemic index, eGI)值。体外实验中,样品在模拟人体胃肠道消化环境中酶解,通过测定并拟合样品碳水化合物的体外水解曲线,最终计算得到样品的eGI值。由于该方法具有复制简易、所需时间短和成本低等优势,在企业研发阶段进行前期原料和配方筛选时比较实用。
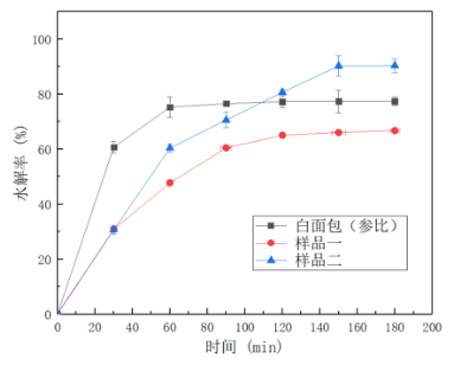
体外消化模型是Englyst[1]率先提出的,他定义了快消化淀粉(Rapidly digestible starch, RDS)、慢消化淀粉(Slowly digestible starch, SDS)和抗性淀粉(Resistant starch, RS)的概念,并建立了一种体外模拟预测食物GI的方法。通过加入唾液淀粉酶、胃蛋白酶、胰酶和葡萄糖苷酶,分别模拟口腔咀嚼、胃部消化和小肠酶解,测定水解0、30、60、90、120、150、180 min时水解液中的葡萄糖浓度,计算得到淀粉在不同时间点的水解率,并绘制样品的水解率曲线如右图,再通过比较样品水解率曲线下面积与参比样品的水解率曲线下面积,得到水解指数(Hydrolysis index, HI),根据eGI与HI的关系式计算得到eGI值。
GI=39.71+0.549HI[2],或者 GI=0.862HI+8.198[3]。
后续的体外消化模型大都是在建立在Englyst的基础上进行改进,不同研究者测试不同原料时建立的消化模型不尽相同,均是为了使体外消化的模型能更加准确地模拟该食物在体内的消化过程和特点。
体外模拟与体内测试相比具有简捷易行的优势,使用少量的样品即可进行测试,可大量筛选不同的原料,为低GI产品的开发做好前期的质量保证。研究表明,样品中的可消化碳水化合物含量越高,其eGI值与体内测试相关性也就越好。但体外测试结果不可以进行GI声称,只有体内测试得到的结果才是真正的食物GI值。
参考文献:
[1] Jenkins DJA, Wolever TMS, Jenkins AL, et al. The glycemic response to carbohydrate foods. Lancet, 1984, 2: 3
[2] Anette E B, Monika T, Gunhild H, et al. Glycemic index in the diet of European outpatients with type 1 diabetes: relations to glycated hemoglobin and serum lipids[J]. American Journal of Clinical Nutrition, 2001, 73(3):574-581.
[3] Bell K J, Smart C E, Steil G M, et al. Impact of fat, protein, and glycemic index on postprandial glucose control in type 1 diabetes: implications for intensive diabetes management in the continuous glucose monitoring era[J]. Diabetes Care, 2015, 38(6):1008-1015.
[4] Buyken A E, Toeller M, Heitkamp G, et al. Carbohydrate sources and glycaemic control in type 1 diabetes mellitus[J]. Diabetic Medicine, 2001, 17(5):351-359.
[5] Dong J Y, Zhang L, Zhang Y H, et al. Dietary glycaemic index and glycaemic load in relation to the risk of type 2 diabetes: a meta-analysis of prospective cohort studies[J]. British Journal of Nutrition, 2011, 106(11):1649-1654.
[6] Stratton, I M. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study[J]. BMJ, 2000, 321(7258):405-412.
[7] Wei J, Heng W, Gao J. Effects of low glycemic index diets on gestational diabetes mellitus: a meta-analysis of randomized controlled clinical trials[J]. Medicine, 2016, 95(22): 1-7.
[8] Viana L V, Gross J L, Azevedo M J. Dietary Intervention in Patients with gestational diabetes mellitus: A systematic review and meta-analysis of randomized clinical trials on maternal and newborn outcomes[J]. Diabetes Care, 2014, 37(12):3345-3355.

